Summary: Accountable Care Organizations (ACOs) are gaining in popularity as a result of the Affordable Care Act. Have you considered the benefits of ACOs from both the patient and provider perspectives?
One of the goals of the Affordable Care Act (ACA) is to provide coordinated care which, in turn, increases quality and efficiency within the healthcare field, and reduces costs.
ACOs – What is an ACO?
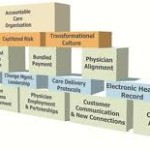
ACOs are groups of providers which form an organization based upon the Medical Home (or PCMH) concept. The Medical Home places responsibility for the coordination of care with the primary physician. The primary care physician coordinates with other physicians and providers such as specialty physicians, laboratories and diagnostic imaging, providing a central point for the patient’s medical information.